CONTRAINDICATIONS
- Serious hypersensitivity reaction to INVOKANA®, such as anaphylaxis or angioedema
WARNINGS AND PRECAUTIONS
-
Diabetic Ketoacidosis in Patients with Type 1 Diabetes Mellitus and Other Ketoacidosis: In patients with type 1 diabetes mellitus, INVOKANA® significantly increases the risk of diabetic ketoacidosis, a life-threatening event, beyond the background rate. In placebo-controlled trials of patients with type 1 diabetes mellitus, the risk of ketoacidosis was markedly increased in patients who received SGLT2 inhibitors compared to placebo; this risk may be greater with higher doses of INVOKANA®. INVOKANA® is not indicated for glycemic control in patients with type 1 diabetes mellitus.
Type 2 diabetes mellitus and pancreatic disorders are also risk factors for ketoacidosis. There have been postmarketing reports of fatal events of ketoacidosis in patients with type 2 diabetes mellitus using SGLT2 inhibitors, including INVOKANA®.
Precipitating conditions for diabetic ketoacidosis or other ketoacidosis include acute febrile illness, reduced caloric intake, ketogenic diet, surgery, insulin dose reduction, volume depletion, and alcohol abuse.
Signs and symptoms are consistent with dehydration and severe metabolic acidosis and include nausea, vomiting, abdominal pain, generalized malaise, and shortness of breath. Blood glucose levels at presentation may be below those typically expected for diabetic ketoacidosis (eg, less than 250 mg/dL). Ketoacidosis and glucosuria may persist longer than typically expected. Urinary glucose excretion persists for 3 days after discontinuing INVOKANA®; however, there have been postmarketing reports of ketoacidosis and glucosuria lasting greater than 6 days and some up to 2 weeks after discontinuation of SGLT2 inhibitors.
Consider ketone monitoring in patients at risk for ketoacidosis if indicated by the clinical situation. Assess for ketoacidosis regardless of presenting blood glucose levels in patients who present with signs and symptoms consistent with severe metabolic acidosis. If ketoacidosis is suspected, discontinue INVOKANA®, promptly evaluate, and treat ketoacidosis, if confirmed. Monitor patients for resolution of ketoacidosis before restarting INVOKANA®.
Withhold INVOKANA®, if possible, in temporary clinical situations that could predispose patients to ketoacidosis. Resume INVOKANA® when the patient is clinically stable and has resumed oral intake.
-
Lower-Limb Amputation: An increased risk of lower-limb amputations associated with INVOKANA® use versus placebo was observed in CANVAS (5.9 vs 2.8 events per 1000 patient-years) and CANVAS-R (7.5 vs 4.2 events per 1000 patient-years), two randomized, placebo-controlled trials evaluating patients with type 2 diabetes who had either established cardiovascular disease or were at risk for cardiovascular disease. The risk of lower-limb amputations was observed at both the 100-mg and 300-mg once-daily dosage regimens.
Amputations of the toe and midfoot (99 out of 140 patients with amputations receiving INVOKANA® in the two trials) were the most frequent; however, amputations involving the leg, below and above the knee, were also observed (41 out of 140 patients with amputations receiving INVOKANA® in the two trials). Some patients had multiple amputations, some involving both lower limbs.
Lower-limb infections, gangrene, and diabetic foot ulcers were the most common precipitating medical events leading to the need for an amputation. The risk of amputation was highest in patients with a baseline history of prior amputation, peripheral vascular disease, and neuropathy.
Before initiating INVOKANA®, consider factors in the patient history that may predispose to the need for amputations, such as a history of prior amputation, peripheral vascular disease, neuropathy, and diabetic foot ulcers. Counsel patients about the importance of routine preventative foot care. Monitor patients for signs and symptoms of infection (including osteomyelitis), new pain or tenderness, sores, or ulcers involving the lower limbs, and discontinue if these complications occur.
-
Volume Depletion: INVOKANA® can cause intravascular volume contraction, which may sometimes manifest as symptomatic hypotension or acute transient changes in creatinine. There have been postmarketing reports of acute kidney injury which are likely related to volume depletion, some requiring hospitalizations and dialysis, in patients with type 2 diabetes mellitus receiving SGLT2 inhibitors, including INVOKANA®. Patients with impaired renal function (eGFR less than 60 mL/min/1.73 m2), elderly patients, or patients on loop diuretics may be at increased risk for volume depletion or hypotension. Before initiating INVOKANA® in patients with one or more of these characteristics, assess and correct volume status. Monitor for signs and symptoms of volume depletion after initiating therapy.
-
Urosepsis and Pyelonephritis: Serious urinary tract infections, including urosepsis and pyelonephritis, requiring hospitalization have been reported in patients receiving INVOKANA®. Treatment with INVOKANA® increases this risk. Evaluate for signs and symptoms and treat promptly.
-
Hypoglycemia With Concomitant Use With Insulin and Insulin Secretagogues: Insulin and insulin secretagogues are known to cause hypoglycemia. INVOKANA® may increase the risk of hypoglycemia when combined with insulin or an insulin secretagogue. Therefore, a lower dose of insulin or insulin secretagogue may be required to minimize the risk of hypoglycemia when used in combination with INVOKANA®.
-
Necrotizing Fasciitis of the Perineum (Fournier’s Gangrene): Necrotizing fasciitis of the perineum, a rare but serious and life-threatening necrotizing infection requiring urgent surgical intervention, has been identified in postmarketing surveillance in female and male patients with diabetes mellitus receiving SGLT2 inhibitors, including INVOKANA®. Serious outcomes have included hospitalization, multiple surgeries, and death. If suspected, start treatment immediately with broad-spectrum antibiotics and, if necessary, surgical debridement. Discontinue INVOKANA®.
-
Genital Mycotic Infections: INVOKANA® increases risk of genital mycotic infections, especially in uncircumcised males or patients with prior infections. Monitor and treat appropriately.
-
Hypersensitivity Reactions: Hypersensitivity reactions, including angioedema and anaphylaxis, were reported with INVOKANA®; these reactions generally occurred within hours to days after initiation. If reactions occur, discontinue INVOKANA®, treat, and monitor until signs and symptoms resolve.
-
Bone Fracture: Increased risk of bone fracture, occurring as early as 12 weeks after treatment initiation, was observed in patients using INVOKANA®. Prior to initiation, consider factors that contribute to fracture risk.
DRUG INTERACTIONS
-
UGT Enzyme Inducers: UGT enzyme inducers (eg, rifampin, phenytoin, phenobarbital, ritonavir) decrease canagliflozin exposure which may reduce the effectiveness of INVOKANA®. For patients with eGFR ≥60 mL/min/1.73 m2, if an inducer of UGTs is administered with INVOKANA®, increase the dosage to 200 mg daily (taken as two 100-mg tablets) in patients currently tolerating INVOKANA® 100 mg daily. The total daily dosage may be increased to 300 mg daily in patients currently tolerating INVOKANA® 200 mg daily who require additional glycemic control.
For patients with eGFR <60 mL/min/1.73 m2, if an inducer of UGTs is administered with INVOKANA®, increase the dose to 200 mg daily (taken as two 100-mg tablets) in patients currently tolerating INVOKANA® 100 mg daily. Consider adding another antihyperglycemic agent in patients who require additional glycemic control.
-
Insulin or Insulin Secretagogues: The risk of hypoglycemia is increased when INVOKANA® is used concomitantly with insulin secretagogues (eg, sulfonylurea) or insulin. Concomitant use may require a lower dosage of the insulin secretagogue of insulin to reduce the risk of hypoglycemia.
-
Digoxin: Canagliflozin increases digoxin exposure. Monitor patients taking INVOKANA® with concomitant digoxin for a need to adjust the dosage of digoxin.
-
Lithium: Concomitant use of an SGLT2 inhibitor with lithium may decrease serum lithium concentrations. Monitor serum lithium concentration more frequently during INVOKANA® initiation and dosage changes.
Drug/Laboratory Test Interference
-
Positive Urine Glucose Test: SGLT2 inhibitors increase urinary glucose excretion which will lead to positive urine glucose tests. Monitoring glycemic control with urine glucose tests is not recommended in patients taking SGLT2 inhibitors. Use alternative methods to monitor glycemic control.
-
Interference With 1,5-Anhydroglucitol (1,5-AG) Assay: Measurements of 1,5-AG are unreliable in assessing glycemic control in patients taking SGLT2 inhibitors. Monitoring glycemic control with 1,5-AG assay is not recommended in patients taking SGLT2 inhibitors. Use alternative methods to monitor glycemic control.
USE IN SPECIFIC POPULATIONS
-
Pregnancy: INVOKANA® is not recommended in pregnant women, especially during the second and third trimesters.
-
Lactation: INVOKANA® is not recommended while breastfeeding.
-
Pediatric Use: Safety and effectiveness in patients <18 years of age have not been established.
-
Geriatric Use: Patients ≥65 years had a higher incidence of adverse reactions related to reduced intravascular volume, particularly with the 300-mg dose; more prominent increase in the incidence was seen in patients who were ≥75 years. Smaller reductions in HbA1c relative to placebo were seen in patients ≥65 years.
-
Renal Impairment: The efficacy and safety of INVOKANA® for glycemic control were evaluated in a trial that included patients with moderate renal impairment (eGFR 30 to <50 mL/min/1.73 m2). These patients had less overall glycemic efficacy, and patients treated with 300 mg per day had increases in serum potassium, which were transient and similar by the end of the study. Patients with renal impairment using INVOKANA® for glycemic control may be more likely to experience hypotension and may be at a higher risk for acute kidney injury.
Efficacy and safety studies with INVOKANA® did not enroll patients with ESKD on dialysis or patients with an eGFR less than 30 mL/min/1.73 m2.
-
Hepatic Impairment: INVOKANA® has not been studied in patients with severe hepatic impairment and is not recommended in this population.
OVERDOSAGE
- In the event of an overdose, contact the Poison Control Center and employ the usual supportive measures.
ADVERSE REACTIONS
- The most common adverse reactions (5% or greater incidence) were female genital mycotic infections, urinary tract infections, and increased urination.
Please read full Prescribing Information and Medication Guide for INVOKANA®.
Canagliflozin is licensed from Mitsubishi Tanabe Pharma Corporation.
cp-68813v8

")
")
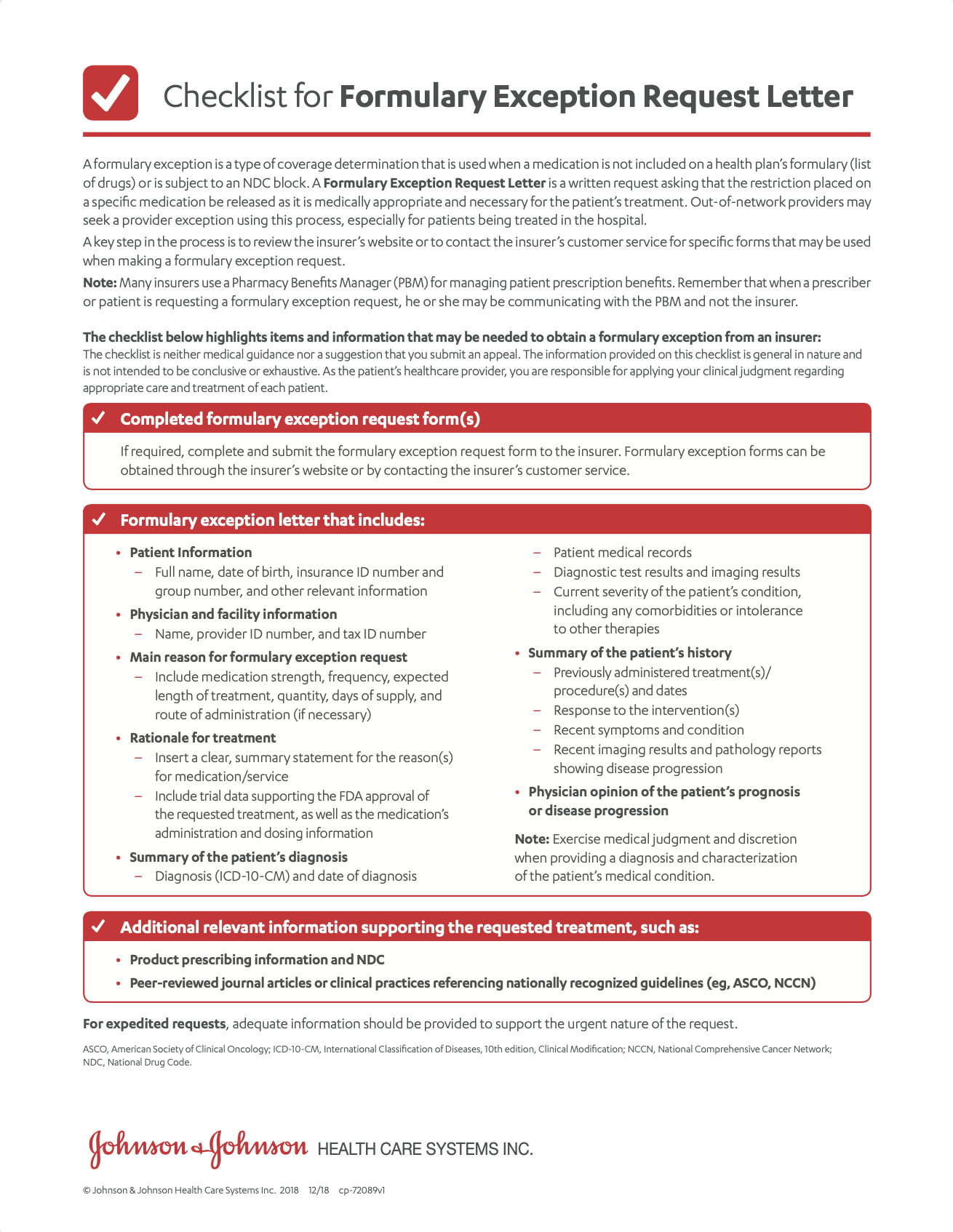
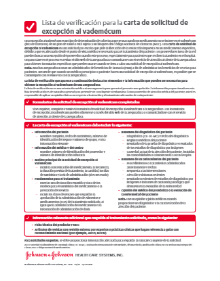



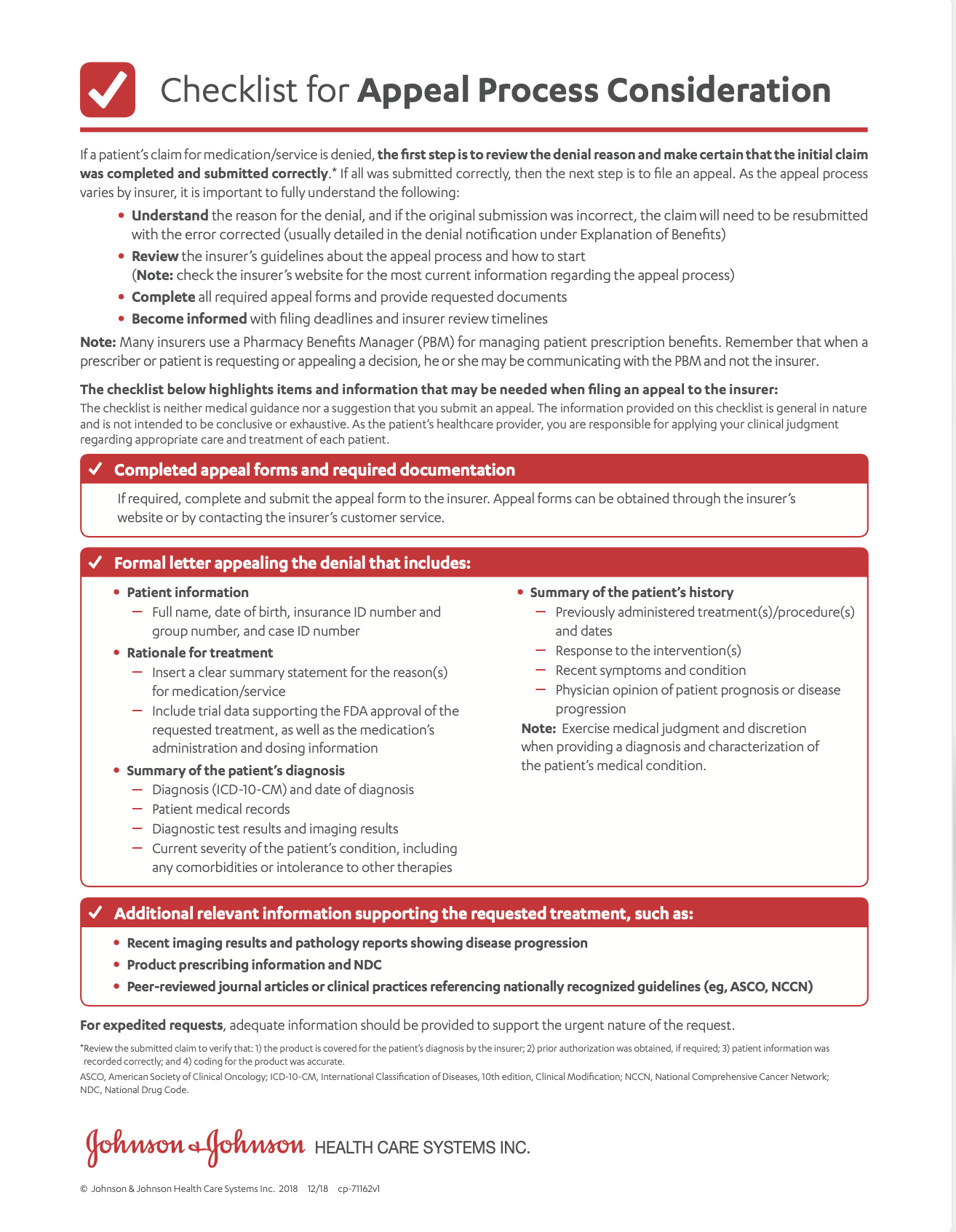
 A template that you can fill out and submit to a patient’s health insurance provider asking them to cover a medication that is not on formulary.
A template that you can fill out and submit to a patient’s health insurance provider asking them to cover a medication that is not on formulary. A template that you can fill out and submit to a patient’s health insurance provider. You may use it to explain why INVOKANA® is medically necessary for your patient.
A template that you can fill out and submit to a patient’s health insurance provider. You may use it to explain why INVOKANA® is medically necessary for your patient.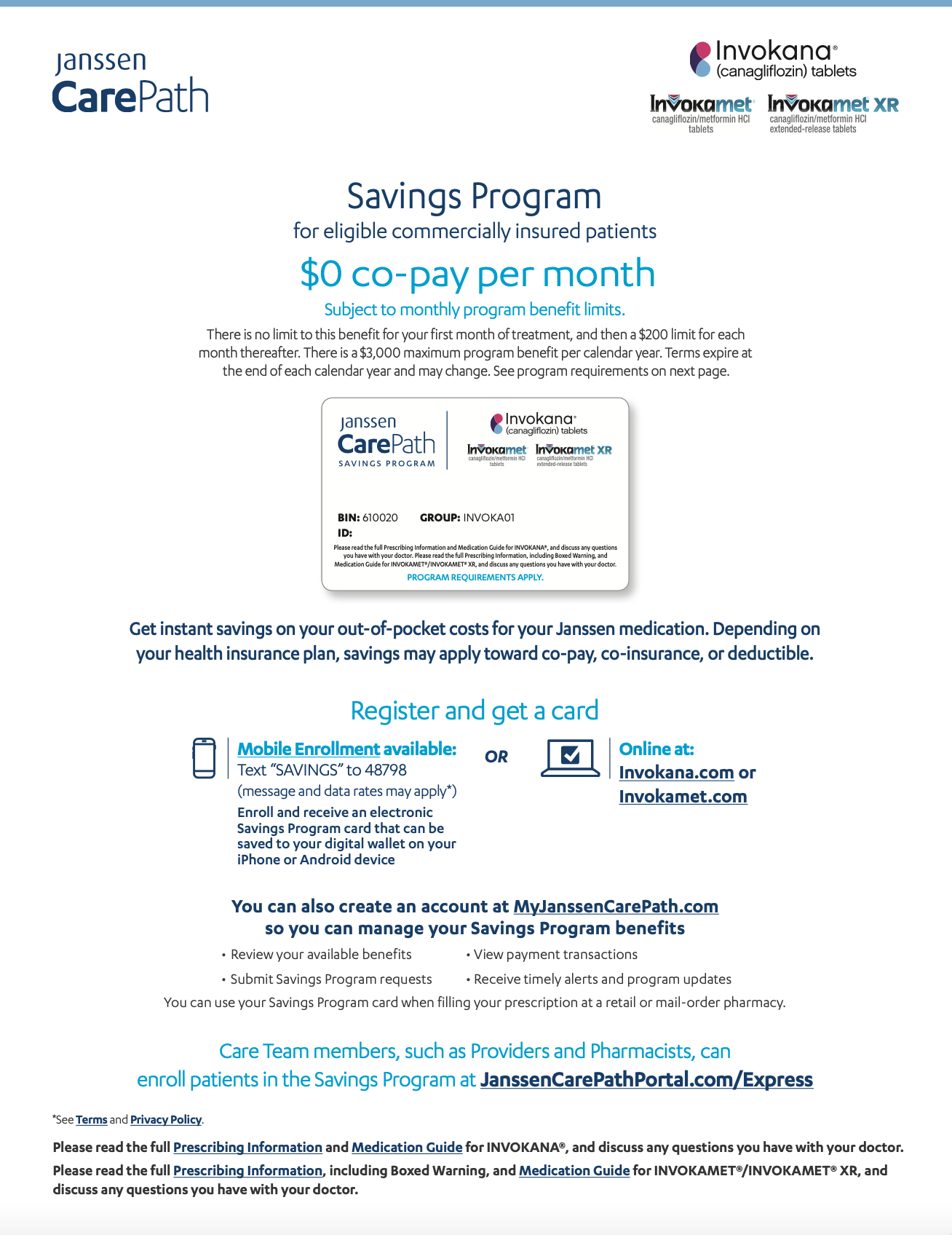 Eligible patients using commercial or private insurance can save on out-of-pocket costs for INVOKANA®.
Eligible patients using commercial or private insurance can save on out-of-pocket costs for INVOKANA®.